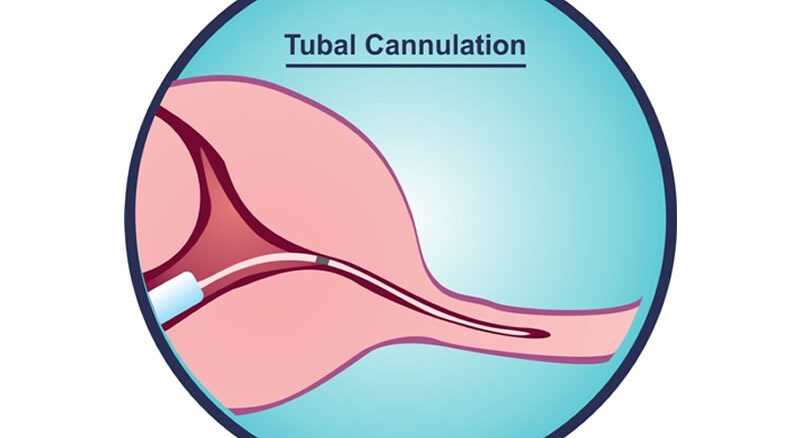
Fallopian tube cannulation is a surgical procedure aimed at opening proximal tubal occlusion in the fallopian tube (blockage in the part of the fallopian tubes closest to the womb). Fallopian tube blockage is a common cause of infertility in women.
It is usually indicated for women with proximal tubal occlusion caused by:
- Mucus plugs at the proximal end of the fallopian tube.
- Minor adhesion at the proximal tube
WHAT TO EXPECT
A hysteroscope will be inserted through the vagina and into the uterus and attached to a monitor to look at the lining of the uterus. Fluid [Normal saline] will be used to distend the cavity of the uterus so the walls can be visualized. The occluded end of the tube is cannulated approximately 1-2 cm with a flexible tubal catheter. Methylene blue is then injected through the cannula and observed for its spillage through the fimbrial end by the surgical assistant performing the laparoscopy. If the tubes are not patent, the assistant straightens the fallopian tube as the hysteroscopic surgeon slides a guidewire with a soft, flexible tip through the initial catheter and into the isthmic area of the fallopian tube. The wire is then withdrawn and patency is evaluated again.
HOW TO PREPARE FOR PROCEDURE
Your doctor will counsel you before the procedure and you will need to give informed consent before the procedure. He would counsel you on the procedure and risks involved. The night before the procedure you will be told not to take any meals from midnight. The anaesthetist would review you and ask questions to assess your risk for anaesthesia. On the morning of the procedure, you can take a shower before you are wheeled into the theatre.
Usually, the procedure lasts 15 – 20 minutes and then you will be discharged once you have fully recovered from the effect of anaesthesia.
