This procedure involves breaking down adhesions within the uterine cavity which could have resulted from repeated dilatation and curettage (D & C), postpartum infection.
It is usually indicated for women with intrauterine adhesion causes by:
- Repeated dilatation and curettage.
- A client who had myomectomy with breaching of the endometrial cavity resulting in adhesions
- A client with septic abortion resulting in adhesions
- Clients with pelvic tuberculosis
WHAT TO EXPECT
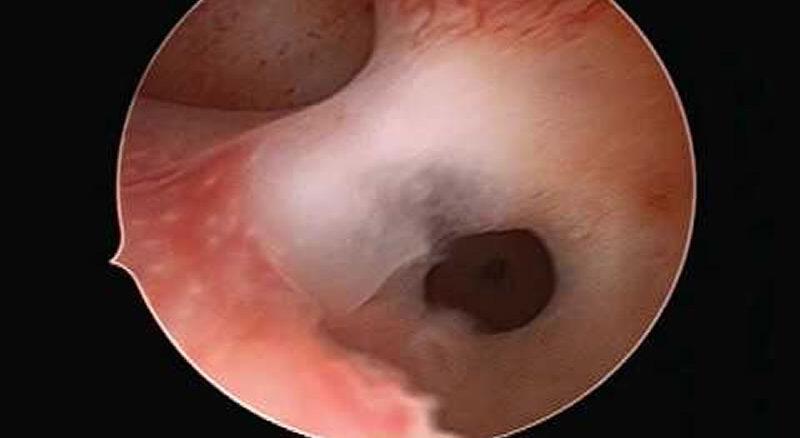
A hysteroscope will be inserted through the vagina and into the uterus and attached to a monitor to look at the lining of the uterus. Fluid [Normal saline] will be used to distend the cavity of the uterus so the walls can be visualized. Hysteroscopic scissors can be used to divide the adhesions and an IUCD or Foley catheter inserted into the cavity to separate the walls. Estrogen and progesterone are given after the procedure to improve endometrial regeneration and antibiotic given for pain.
Follow-up hysterosalpingography [HSG] or diagnostic hysteroscopy after withdrawal bleeding or 6 – 8 weeks after the procedure is recommended.
HOW TO PREPARE FOR PROCEDURE
Your doctor will counsel you before the procedure and you will need to give informed consent before the procedure. He would counsel you on the procedure and risks involved. The night before the procedure you will be told not to take any meals from midnight. The anaesthetist would review you and ask questions to assess your risk for anaesthesia. On the morning of the procedure, you can take a shower before you are wheeled into the theatre.
Usually, the procedure lasts 20 – 30 minutes and then you will be discharged once you have fully recovered from the effect of anaesthesia.
