INTRODUCTION
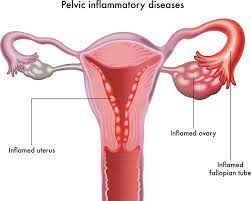
PID is described as an infection of the female genital tract which begins from the uterus, spreading to the fallopian tubes and other pelvic structures such as the ovary. It is a serious infection and if not treated promptly could cause damage to the fallopian tube leading to infertility in women.
Single infection with PID increases the risk of tubal damage by 18%, with a 2nd infection the risk increases to 34% and a 3rd infection by 50 – 60 %.
Persons who run the risk of acquiring PID include:
- ladies with multiple sexual partners,
- lack of use of condom during sex in a lady with multiple sexual partners or where her partner has multiple partners,
- a young girl engaging in sex and
- smoking of cigarettes.
- women using IUCD
- women with immunosuppressive diseases such as HIV
SYMPTOMS
A lady with PID could present with no symptoms. When symptoms occur they could include the following.
- Abdominal pains in the lower region making sexual intercourse unbearable.
- Vaginal discharge which could have an unpleasant smell
- Fever [lady feels her body is hot]
- Spotting from the vagina
- Pains during urination [dysuria]
CAUSES
PID is usually caused by several bacteria organisms especially those that are transmitted sexually. While it is common in young girls with multiple sexual partners, women with Intrauterine Contraceptive Device [IUCD] for family planning also have an increased risk of acquiring the infection.
Organisms that could cause PID include:
- Neisseria gonorrhoea [cause of gonorrhoea]
- Chlamydia trachomatis
- Escherichia coli [E coli]
- Streptococcus
PREVENTION
The risk of acquiring a PID can be reduced by:
- Being faithful to one faithful partner
- Use a condom if you’re having casual sex
- Delay sexual intercourse until you are older as a lady
- If you have an IUCD inserted, see your doctor regularly
- Get tested if you feel you have a PID
- Have your partner tested if you have been infected with a sexually transmitted disease
COMPLICATIONS
If PID is not treated it could lead to long term challenges in the woman. These include:
- Infertility
Infertility arises as a result of damage to the fallopian tubes of the woman by the offending organism. After 3 PID infections, the risk of tubal damage rises by more than 50 %.
- Tubo-ovarian abscess
A tubo-ovarian abscess is a collection of pus in the fallopian tube and ovary which forms as a result of infection with PID. Left untreated, it could lead to severe life-threatening infection with the possibility of reverting to surgery.
- Ectopic pregnancy
Damage to the fallopian tube could lead to scar tissue formation which could cause a fertilized egg to get trapped within the tube while trying to make its way to implant in the uterus. Unrecognized, ruptured ectopic pregnancy could lead to massive intra-abdominal bleeding and death.
- Chronic pelvic pain
This occurs in 2 out of every 10 patients with a history of PID. The pains usually last for 6 months to several years and could be due to adhesion formation between organs.
DIAGNOSIS
Diagnosing PID usually begins with a history of recent unprotected sexual intercourse and the symptoms which have been mentioned above.
At the health facility, your doctor may perform a general examination and elicit pains in your abdomen. Pelvic examination may reveal offensive vaginal discharge with pains when the cervix is touched [cervical motion tenderness].
Laboratory examination done may include:
- Endocervical Swab test for microscopy, culture, and sensitivity which may reveal a large number of pus cells and the organism involved
- Full Blood Count which shows a high white blood cell count
A transvaginal scan may be useful in cases of tubo-ovarian abscess or hydrosalpinx.
Laparoscopy may also be carried out to have a good view of the pelvic organs and to collect a specimen for culture. It involves inserting a laparoscope through the abdomen to visualize the pelvis.
TREATMENT
When a doctor makes a diagnosis of PID, the client will be placed on several medications.
Medical Treatment
Involves the use of antibiotics probable intravenous or intramuscular. Antibiotics help prevent possible complications.
Surgery
This may become necessary in some cases when there is an abscess [pus] collection in the tubes and ovaries. Most times, it will be performed after a course of antibiotics for drainage of the abscess. This could be carried out through Laparoscopy [involves the use of pinhole incisions with the aid of a camera to access the abdominal cavity] or Laparotomy [involves making a large incision through the abdominal wall to gain access into the cavity].
Laparoscopy is the favoured option of management as it is minimally invasive and reduces the risk of further adhesions among other benefits.
Partner[s] Treatment
This involves contact tracing to identify sexual partners and get them treated if necessary. Treatment of partner[s] helps protect them and prevent future reinfection.
WHEN TO SEE A DOCTOR
You are advised to see your doctor if you experience the following.
- If you suspect your partner has a sexually transmitted infection or is treating himself for one
- If you have abnormal offensive vaginal discharge
- If you have severe lower abdominal pains
- If you have a fever accompanied by vomiting
- If you have pains during sexual intercourse
- If you have pains while urinating
